


 Sign Out
Sign Out

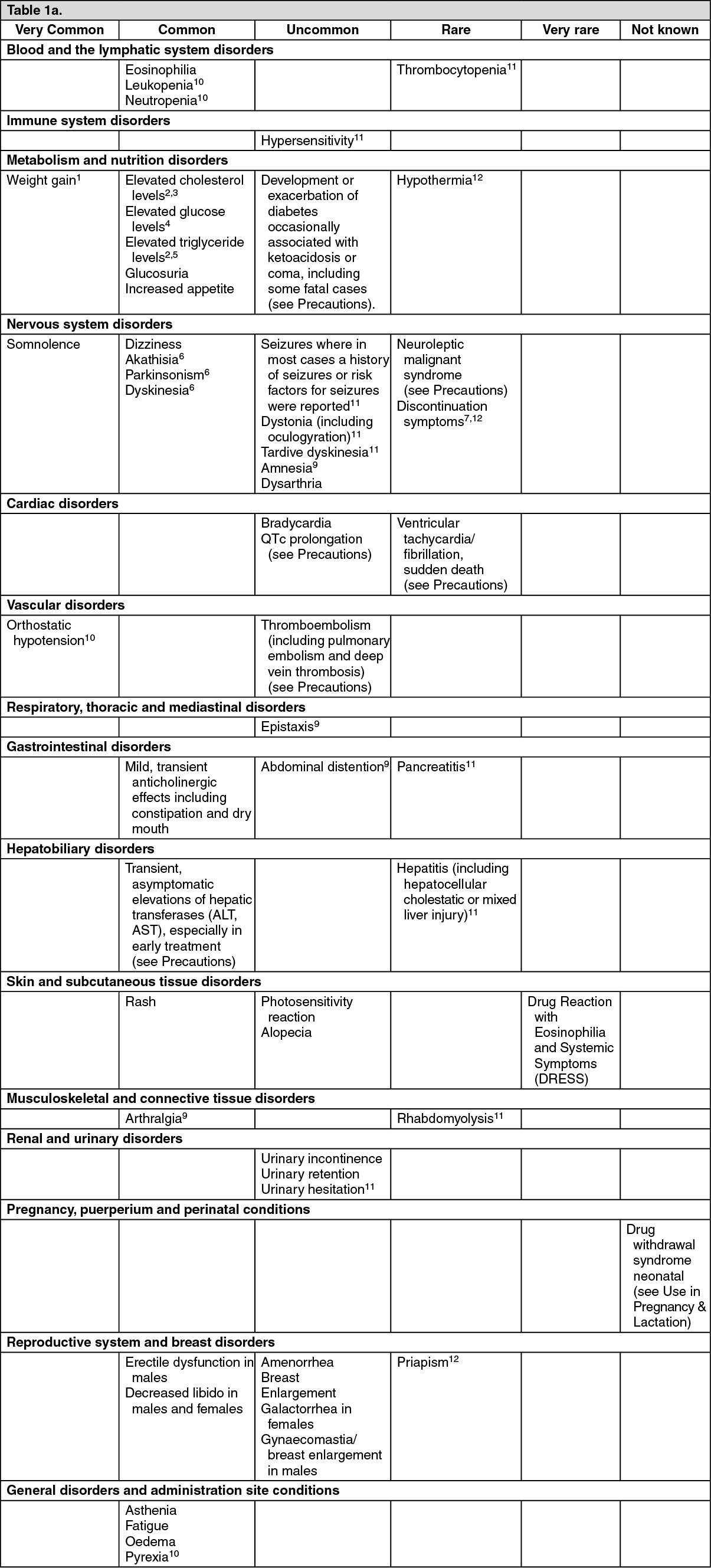
Tabulated list of adverse reactions: The following table lists the adverse reactions and laboratory investigations observed from spontaneous reporting and in clinical trials. Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. The frequency terms listed are defined as follows: Very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to< 1/1,000), very rare (< 1/10,000), not known (cannot be estimated from the data available). (See Table 1A and Table 1B.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image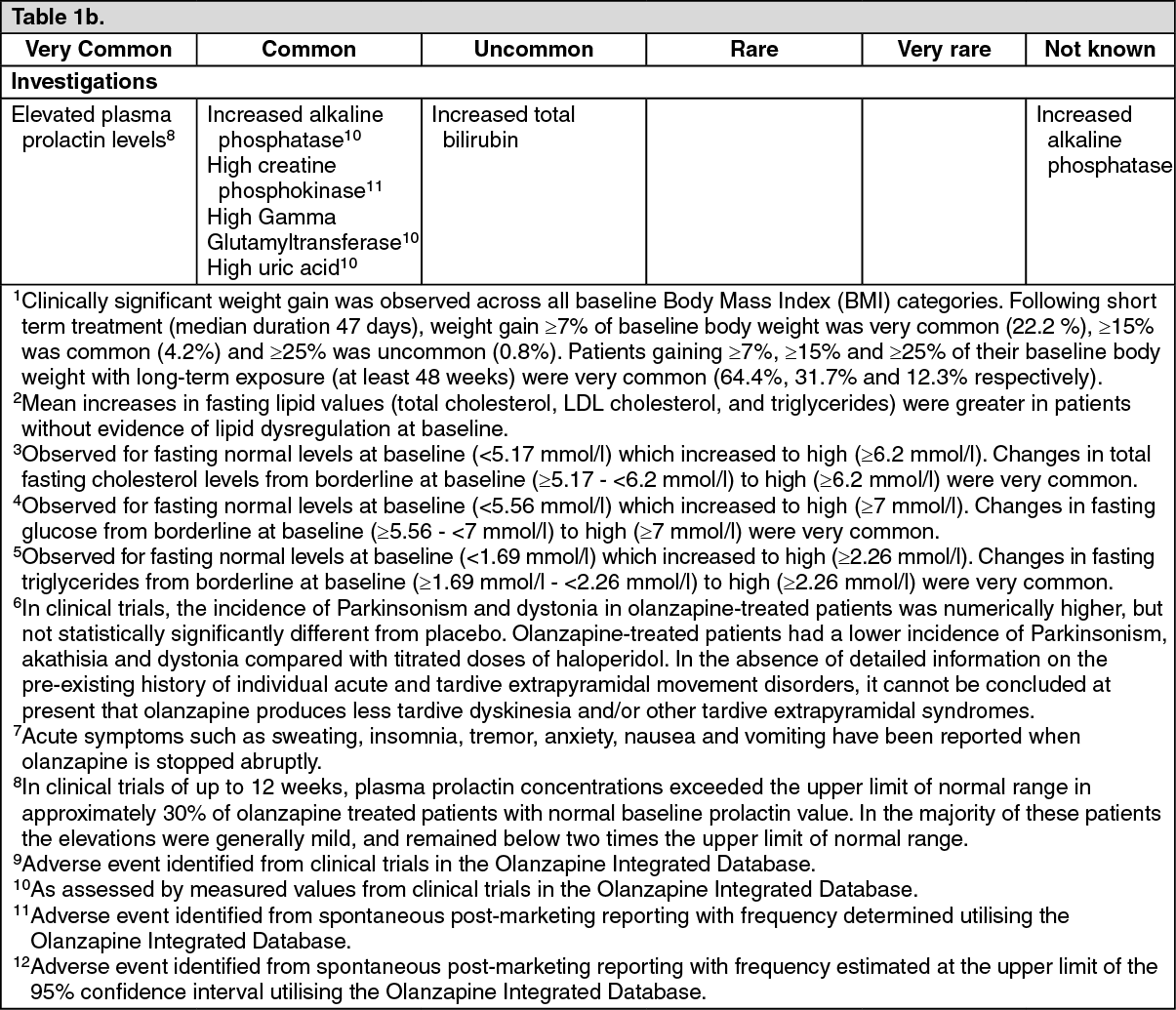 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLong-term exposure (at least 48 weeks): The proportion of patients who had adverse, clinically significant changes in weight gain, glucose, total/LDL/HDL cholesterol or triglycerides increased over time. In adult patients who completed 9-12 months of therapy, the rate of increase in mean blood glucose slowed after approximately 6 months.
Additional information on special populations: In clinical trials in elderly patients with dementia, olanzapine treatment was associated with a higher incidence of death and cerebrovascular adverse reactions compared to placebo (see Precautions). Very common adverse reactions associated with the use of olanzapine in this patient group were abnormal gait and falls. Pneumonia, increased body temperature, lethargy, erythema, visual hallucinations and urinary incontinence were observed commonly.
In clinical trials in patients with drug-induced (dopamine agonist) psychosis associated with Parkinson’s disease, worsening of Parkinsonian symptomatology and hallucinations were reported very commonly and more frequently than with placebo.
In one clinical trial in patients with bipolar mania, valproate combination therapy with olanzapine resulted in an incidence of neutropenia of 4.1%; a potential contributing factor could be high plasma valproate levels. Olanzapine administered with lithium or valproate resulted in increased levels (≥10%) of tremor, dry mouth, increased appetite, and weight gain. Speech disorder was also reported commonly. During treatment with olanzapine in combination with lithium or divalproex, an increase of ≥ 7% from baseline body weight occurred in 17.4% of patients during acute treatment (up to 6 weeks). Long-term olanzapine treatment (up to 12 months) for recurrence prevention in patients with bipolar disorder was associated with an increase of ≥7% from baseline body weight in 39.9% of patients.
Paediatric population: Olanzapine is not indicated for the treatment of children and adolescent patients below 18 years. Although no clinical studies designed to compare adolescents to adults have been conducted, data from the adolescent trials were compared to those of the adult trials.
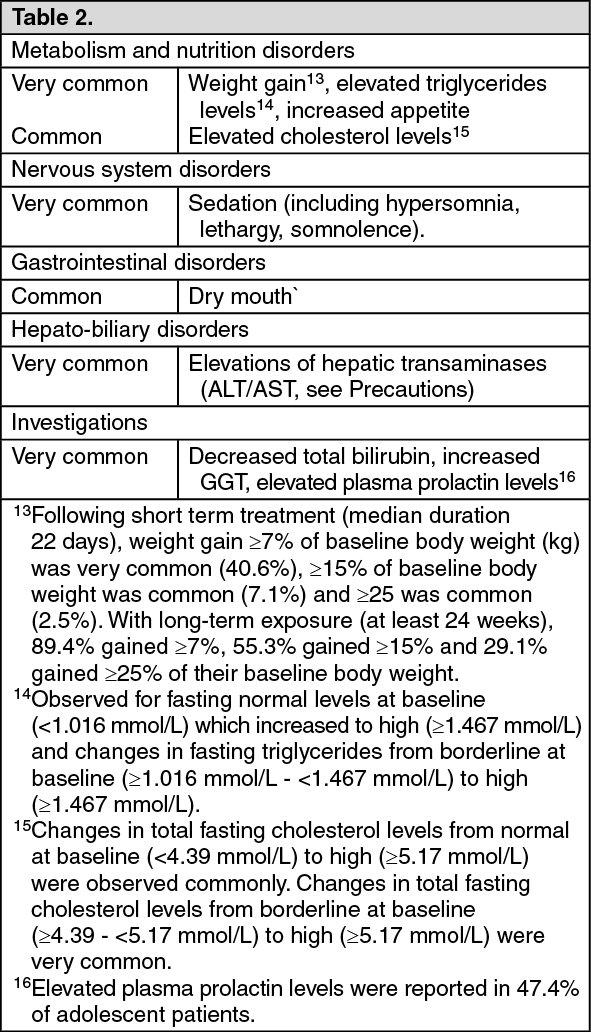
The following table summarises the adverse reactions reported with a greater frequency in adolescent patients (aged 13-17 years) than in adult patients or adverse reactions only identified during short- term clinical trials in adolescent patients. Clinically significant weight gain (≥ 7%) appears to occur more frequently in the adolescent population compared to adults with comparable exposures. The magnitude of weight gain and the proportion of adolescent patients who had clinically significant weight gain were greater with long-term exposure (at least 24 weeks) than with short-term exposure.
Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness. The frequency terms listed are defined as follows: Very common (≥ 1/10), common (≥ 1/100 to < 1/10). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form